

My breast cancer screening journey
We deserve better

Six months ago, I was in good spirits when I checked in for a routine breast cancer screening mammogram. It’s not fun to have your breasts squeezed between two chilly plates, but I’m deeply committed to proactive healthcare. I’m the type of person who religiously shows up for dental checkups, Pap smears, vaccines, and anything else that gets me ahead of potential health issues.

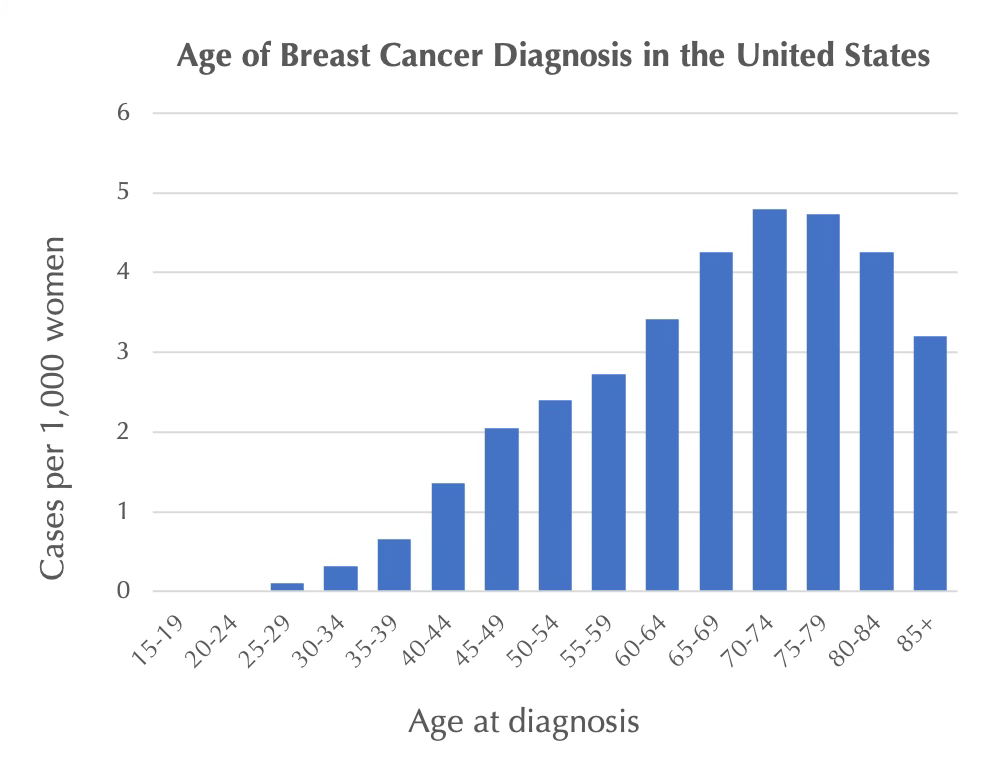
After my first mammogram at age 45, I received a reassuring bill of health, and I expected the same outcome this time. Breast cancer is rare in 40-something women of average risk like myself, and I’m not normally one to worry about unlikely events.
Roughly 2 to 4 cancers are detected per 1,000 average-risk women screened in their forties, according to this study and the BC Cancer Agency decision tool.
Over 10 years, screening mammography will detect 20 breast cancers per 1,000 women in their forties, according to Canadian Task Force on Preventative Health Care.
At the same time, I knew there was a decent chance of being called back for more testing, only to learn that it was not cancer (false positive). False alarms are an inevitable part of any screening program. If we want to catch as many cancers as possible, we must be willing to investigate results that are slightly suspicious (but often turn out to be fine).
After a routine screening mammogram, roughly 1 in 10 women are called back for further evaluation in the United States and Canada. Over 90% of these recalls are false alarms, known as “false positives” - not cancer.
Over 10 years of screening in women in their forties, more than half will experience at least one false-positive recall and roughly 7 in 100 will have an unnecessary biopsy (see this US study and HealthLink British Columbia).
As I awaited my results, I was feeling optimistic, relaxed, and pleased about my proactiveness. This changed abruptly when I received my results: a voicemail from the screening center asking me to come in for follow up testing. I listened to the message twice, shocked by the outcome (this isn’t supposed to happen to me!), the meagre contents (no context), and the impersonal delivery of this type of news.
My data-driven mindset went out the window, replaced by anxious thoughts. What if I’m one of the unlucky ones? What treatment will I need? How will my family manage? How will I manage? I eventually received a letter from the BC Breast Cancer Screening Program explaining that most recalls are false alarms, but the whole communication experience still felt woefully lacking.
The soonest available follow up appointment was two months away. This seemed crazy but is apparently par for the course here in British Columbia, ever since the COVID pandemic wreaked havoc. I took some comfort in the fact that that my long delay likely reflected a low urgency assessment, as our system responds better to acute crises. I found myself thinking of others who didn’t receive reassuring information in an accessible format, or were simply more prone to anxiety than me.
One of the best things I did while in limbo was to open up about my situation with others. I learned that many of my friends had experienced one or more false positive mammograms. Their stories were even more powerful than the data.

My long-awaited recall appointment went smoothly, including another mammogram and an ultrasound (on account of my higher breast density). I was surprised to be asked back for a third mammogram and another ultrasound, which took place a month later. One week later, my doctor called to tell me that they wanted to do a needle biopsy. She gave me the courtesy of a heads up so that I wouldn’t be surprised by a call from the cancer centre, which I appreciated.
Still, delivery of this biopsy request fell short of what I needed. There was no information package, just a brief phone call. My doctor told me that “the good news is that your case was not labeled as high suspicion”. When I pushed her more for details on possible outcomes, she replied “many biopsies come back negative (not cancer); it’s hard to say how many, maybe 50-50. But let’s not worry yet”. I instantly regretted forcing her into what felt like a wild guess. Was she seriously saying, in a casual way, that there was a 50% chance that I have cancer, while telling me not to worry?!

While waiting six long weeks for my biopsy appointment, I went into scientific detective mode. My mission was to get a rough sense of how often biopsies like mine are diagnosed as cancer rather than something else (e.g. calcification, benign cyst, etc). I found very little public-facing information on this question, which was alarming given that so many people face this stressful situation. The scientific studies that I found were unsettling - they suggested that the chances that I have cancer are probably around 1 in 4 or lower. Personally, I prefer knowing these (very rough) odds to an information void.
One study estimated that 1 in 4 are cancerous (4 of 15) while another study estimated that roughly 1 in 5 biopsies are cancerous in my age group. I assume that these stats include cases that are labeled as “high suspicion”, unlike my own, suggesting that my own odds are more favourable.

My biopsy appointment was earlier this week, and I arrived feeling nervous but excited to finally have clarity. Sadly, things did not go smoothly. I learned that my suspicious spot is in a particularly difficult spot to access. After an uncomfortable aborted attempt, the radiologist referred me to the local cancer agency where specialized equipment should make the biopsy feasible. I’m currently awaiting a call to schedule this biopsy.
Six months into my screening saga, I still don’t know whether or not I have breast cancer, nor do I know when I’ll have the answer. I’m shocked and disappointed by the profoundly inadequate state of the breast screening system in British Columbia. How is it okay to tell someone they may have cancer, without explaining the (favourable) odds, and leave them in limbo for months?
We need much shorter delays, access to clear information at each step, and more acknowledgement of the emotional toll of this journey. I don’t fault the doctors, nurses, and technicians who are doing their best with scarce resources - it’s the system that’s broken.
It feels risky to share my story when it’s still being written, but I wanted it to be raw. My hope is that it helps others who are also in screening limbo, or will be in the future. I want you to know that you’re not alone, and that there are data available to guide you, if you know where to look. I also hope that this message reaches those whose loved ones are going through a screening journey. Data can help, but emotional support is just as important, in my experience.
I encourage you to check out the resources below to learn about the benefits and risks of screening. I also recommend opening up to trusted friends and family if you’re struggling on your journey. It really helps!
I don’t know how I’ll feel about sharing future updates, whatever they may be, but know that I appreciate all of your well wishes.
Yours in science and in heart,
Chana
Note: The stats presented here are from studies of North American cisgender women. The risks and benefits of screening vary greatly depending on the population (e.g. age, race, risk factors and more), the screening technologies, and the overall structure of the screening program. For example, breast cancer screening programs in Europe tend to have lower rates of recalls and false alarms (e.g. recall rates are roughly 4 in 100 according to Cancer Research UK, compared to 10 in 100 in North America). Screening guidelines for other populations are emerging, including transgender, non-binary and two-spirit individuals.
Resources & References
Breast cancer screening decision aid (British Columbia Cancer Agency)
My article on breast cancer screening in your 40s for
The messy math of mammograms (Science Friday)
Breast cancer screening guidelines 2024 (United States Preventative Services Task Force)
Breast cancer screening guidelines 2024 (Canadian Task Force on Preventative Health)
Benefits and Harms of Breast Cancer Screening Mammograms Over 10 years (Canadian Task Force on Preventative Health Care 2024)

Oh, it’s not just Canada. I’m currently navigating this process in the US — nerve wracking how long it takes to get any solid information.
Thank you for sharing this, Chana. My fingers and toes are tightly crossed for you!